To better understand conditions of the knee, lets look at the anatomy of the knee joint and how the parts of the knee work together to maintain normal function.
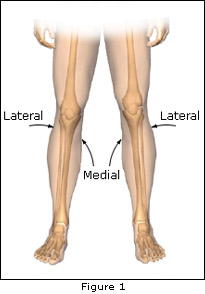
The Medial side of the knee is the side that is closest to the other knee. The lateral side of the knee is the side that is away from the other knee. Structures on the medial side usually have medial as part of their name, such as the medial meniscus. Similarly, structures on the lateral side usually have lateral as part of their name, such as the lateral meniscus.
The important parts of the knee include bones, ligaments, tendons and cartilage. The bones forming the knee joint include: the Femur, the large bone in the thigh, the Tibia, the large bone in the lower leg, the Fibula is the small bone in the lower leg and the patella or knee cap. Two ligaments are found on either side of the knee joint - the Medial Collateral Ligament and the Lateral Collateral Ligament.

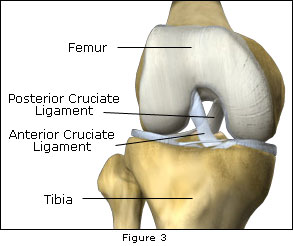
Inside the knee joint, two ligaments span between the femur and the tibia. The Posterior Cruciate Ligament and the Anterior Cruciate Ligament. The posterior cruciate ligament prevents the lower leg bone (tibia) from going posteriorly to the upper leg bone (femur). The anterior cruciate ligament prevents the lower leg bone (tibia) from going anteriorly to the upper leg bone (femur) [figures 3 and 5].
Two structures called Menisci reside between the femur and the tibia. These structures are sometimes referred to as the "cartilages" of the knee [figure 4].
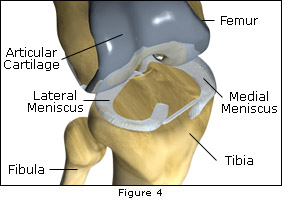

Articular Cartilage, on the other hand, is a white shiny material with a rubbery consistency that covers the end of the femur, the top of the tibia, and the back of the patella. The function of articular cartilage is to absorb shock and provide an extremely smooth bearing surface to facilitate motion.
Finally, the Extensor Mechanism sits in front of the knee joint.(Figure 2) The Patella is the fourth bone of the knee joint. The Patellar Tendon connects the patella to the tibia. This tendon covers the patella and continues up the thigh as the Quadriceps Tendon.
The ligaments of the knee joint are primarily stabilizers of the joint. Most joints in the body have a stable bony configuration. For instance, the hip joint is a ball which sits inside a deep socket. The ankle joint has a shape similar to a mortise. The knee has very little bony stability, and behaves more like a round ball on a flat surface. Because there is no inherent bony stability, the ligaments of the knee are very important for stability. The Medial Collateral and Lateral Collateral Ligaments prevent the knee from moving too far in the side to side direction. The Anterior Cruciate ligament and the Posterior Cruciate ligaments control the front to back motion of the knee joint. The Anterior Cruciate ligament keeps the tibia from sliding too far forward in relation to the femur. The Posterior Cruciate ligaments keep the tibia from sliding to far back in relation to the femur. Working together, the two cruciate ligaments control the back and forth motion of the knee. The ligaments, all taken together, are the most important structures controlling stability of the knee.
The menisci of the knee are important for two reasons:
The menisci actually wrap around the thigh bone to fill the space between the round femur and the flat tibia. The menisci act like gaskets helping to distribute the weight from the femur to the tibia. Without the meniscus, any weight on the femur will be concentrated to one point on the tibia. With the menisci the weight is spread out across tibial surface. Weight distribution by the meniscus is important because it protects the articular cartilage from excessive forces. Without the meniscus, the concentration of force into a small area on the articular cartilage can damage the surface, leading to degeneration over time. How does the meniscus help the ligaments with stability of the knee? The meniscus enhances stability by acting like a chock under a tire, and keeps the round femur from rolling on the flat tibia. In essence, the meniscus converts the tibia surface into a shallow socket. A socket configuration is more stable and more efficient at transmitting the weight bearing forces. Hence, the meniscus enhances the stability of the knee and protects the articular cartilage from excessive concentration of force.
Articular Cartilage covers the ends of the bones that makes up the joint. This material is about ¼ of a inch thick in most large joints. The articular surface is a tough, very slick material that allows the surfaces to slide against one another without damage to either surface. Damage to or loss of articular cartilage is commonly referred to as arthritis.
The Quadriceps Mechanism is the motor that drives the knee joint, and allows us to walk. The Quadriceps Mechanism is composed of the patellar tendon, the patella, and the quadriceps muscle/tendon on the front of the thigh. The patella fits into a groove called the Patellofemoral groove on the front of the femur. The way in which the patella fits into this groove, and slides as the knee bends, can affect the overall function of the knee. The patella functions like a fulcrum, and increases the force exerted by the quadriceps muscle as the knee straightens. When the Quadriceps Muscle contract, the knee straightens. When it relaxes, the knee bends. While this is not a complete anatomy of the knee, it represents a brief discussion of the most common problematic portions of the knee.
The Anterior The Anterior Cruciate Ligament is the most commonly injured ligament of the knee. The ACL controls how far the tibia moves anteriorly in relation to the femur. The major cause of injury to the ACL is sports related. This injury occurs when the knee is forcefully twisted or hyperextended. Many patients recall hearing a loud "pop" when the ligament tears, and they feel the knee give way. Rapid swelling may occur.
The ACL may not be the only ligament injured when the knee is twisted violently. It is not uncommon to have both the Medial Collateral ligament (and/or the Lateral Collateral ligament) and the ACL injured. The menisci (cartilage) of the knee may also be torn. Rarely, the joint surfaces may be damaged.
The symptoms following a tear of the ACL are variable. Usually there is swelling of the knee within a short time following the injury due to bleeding into the knee joint from torn blood vessels in the ligament. The instability caused by the torn ligament leads to a feeling of insecurity and giving way of the knee, especially when trying to change direction on the knee.
The pain and swelling from the initial injury will usually resolve after 2 to 4 weeks, but the instability remains. The symptoms of instability, and the inability for the patient to trust the knee for support are indications for treatment. Also important in the decision about treatment is the growing realization by Orthopaedic Surgeons that long-term instability may lead to arthritis of the knee.
The History and Physical Examination are the most important tools in diagnosing a rupture or deficient ACL. In the acute injury, the swelling is a good indicator. A good rule of thumb is that any tense swelling that occurs within two hours of the knee injury is blood in the joint, this is called a Hemarthrosis. If swelling is marked, draining as much fluid as possible gives relief and provides useful information. If blood is found when draining the knee, there is about a 70% chance the ACL is torn.
An X-ray of the knee to rule out a fracture will also be ordered on the initial examination. While ligaments and tendons do not show up on x-rays, bleeding into a joint also occurs when a fracture into the knee joint is present, or when portions of the joint surface are "chipped off". An x-ray helps to exclude these possibilities.
In some cases, an MRI is obtained to further evaluate the knee injury. The MRI (Magnetic Resonance Imaging) uses magnetic waves rather than x-rays to show the soft tissues of the body. An MRI is able to "slice" through the area and see the anatomy and injuries very clearly. An MRI does not require any needles or special dye, and is painless.
In rare cases, Arthroscopy may be used to make a definitive diagnosis if there is a question about what is causing knee symptoms. Arthroscopy is a type of an operation where a small fiberoptic TV camera is placed into the knee joint, allowing the physician to look at the structures inside the knee joint directly.
When one has an acute injury to their knee and tears their anterior cruciate ligament, the decision of whether or not surgery is indicated involves profiling the patient. Such profiling is done in an attempt to determine which patient is likely to develop functional instability of their knee. Functional instability means that the knee will give way or "slip out" and swell during daily or sports activities. Repeated episodes of instability will result in further damage to the knee and produce arthritis. I have determined that the following seven (7) A's are useful in making the decision regarding whether or not surgery would be the best for one who tears their anterior cruciate ligament.
To restore range-of-motion (ROM), strength, and confidence to the knee while protecting the anterior cruciate ligament (ACL) graft from stretching or rupturing.
The rehabilitation program is a four month, vigorous, structured program. The end-result depends to a great extent on the patients discipline, motivation, and perseverance in performing the exercise program. Without commitment from the patient, the surgery is assured to fail to meet expectations. With cooperation and dedication, the patient has an excellent chance to regain the strength, stability, and confidence in the knee that existed before injury.
Many patients are too busy with the demands of work and family to participate in a formal physical therapy program that requires regular attendance at therapy sessions at inconvenient times during the day. Fortunately, in the majority of cases, rehabilitation can be done at home or while traveling using a stationary bicycle, pool, or exercise equipment at a health club. The following exercise program is a sample program. A detailed protocol will be designed specifically for you, and your trainer or physical therapist.
Your progress will be monitored at each of these visits. Rarely, it may be necessary to perform a manipulation of the knee or an additional arthroscopy to assist you in regaining motion or to remove adhesions.
ROENTGENOGRAMS: An x-ray of your knee is obtained before your visit. The placement of the graft tunnels and fixation devices will be reviewed with you in the office.
Some surgery maybe performed as an outpatient. Patients go home 5-6 hours after surgery when they can eat and walk with crutches. Others stay overnight and are discharged the next day. If you have your own crutches please bring them to the hospital with you.
The surgery usually requires 2 hours to perform. Repairing or removing a torn meniscus can add 15-20 minutes to the operation.
When you feel safe and confident behind the wheel so you can avoid getting into an accident. Generally, driving is often resumed within the first week after surgery, but may take longer if you have to work a clutch. Do not drive when you are taking pain pills.
Motivated people who have a sitting or desk job can usually be back at work or school by 4-5 days after surgery. Construction workers take 4-6 months.
90% of patients will have stability nearly equal to the normal knee and will be able to return to full unrestricted activities.
Of course, remember that you tore your own natural ligament, so it is theoretically possible to rupture THE graft. Fortunately, rupture of the graft is uncommon. You are more likely to tear the ACL in the other knee than to re-tear your reconstructed ligament.
Yes, the therapist can call 274-0960 and let the office know if they would like to observe the surgery. It is a hospital policy the non-medical personal are not permitted in the operating room; this includes family and friends.
If you have any more questions, and you should, please write them down and ask me.
The meniscus is the most commonly injured structure in the knee. The injury can occur in any age group. In younger people, the meniscus is fairly tough, and tears usually occur as a result of a fairly forceful twisting injury. In older people, the meniscus grows weaker with age, and meniscus tears occur as a result of a fairly minor injury, even from the up and down motion of squatting. Remember, there is a meniscus on either side of the knee joint. The meniscus acts like a gasket between the femur and the tibia. The meniscus can be torn in several ways. The entire inner rim of the meniscus can be torn in what is called a bucket handle tear. The meniscus can also have a flap torn from the inner rim, or the tear can be a degenerative type tear where a portion of the meniscus is frayed and torn in multiple directions.
The most common problem caused by a torn meniscus is pain. The pain may be felt along the joint line where the meniscus is located or may be more vague and involve the whole knee. If the torn portion or the meniscus is large enough, "locking" may occur. Locking occurs when the fragment of meniscus gets caught in the hinge mechanism of the knee and will not allow the knee to straighten completely. There are long-term effects of a torn meniscus. The constant rubbing of the torn meniscus on the articular cartilage may cause wear and tear on the surface, leading to arthritis of the joint.
Diagnosis begins with a history and physical examination. The examination will try to determine where the pain is located, whether or not locking has occurred, and if there are any clicks or pops as the knee is moved. X-rays will not show the torn meniscus. They are mainly useful to determine if other conditions are present. An MRI scan is very good at showing the meniscus. If the history and physical examination strongly suggest that a torn meniscus is present, then arthroscopy may be suggested to confirm the diagnosis and treat the problem at the same time. I order MRI's if the clinical history and exam are not absolutely diagnostic of a meniscus tear.
Initial treatment for a torn meniscus is non-operative and directed towards reducing the pain and swelling in the knee. If the symptoms continue, surgery will be required to either remove the torn potion of the meniscus or to repair the tear. Most meniscus surgery today is done using the arthroscope. Small incisions are made in the knee to allow the insertion of a small TV camera into the joint. Through another small incision, special instruments are used to remove the torn portion of meniscus while the arthroscope is used to view the inside of the joint. In some cases, the meniscus tear can be repaired. The arthroscope is used to view the torn meniscus. Sutures are then placed into the torn meniscus. The placement of sutures continues until the tear is repaired. Repair of the meniscus is not possible in most cases. Young people with relatively recent meniscal tears are the most likely candidates for repair. Degenerative type tears in older people are not repairable.
The healthy knee is a hinge joint. The three bones that form the knee are the thighbone (femur), shinbone (tibia), and kneecap (patella). The femur and tibia are held together by ligaments, which are strong bands of tissue that stabilize the joint. The end of the femur, the top of the tibia, and the back of the patella are covered with a tough tissue called articular cartilage. This cartilage acts like a natural shock absorber, preventing both bone on bone contact and providing a smooth, pain-free surface for the bones to glide against. The knee also contains synovial membranes, which produce synovial fluid to help lubricate and nourish the articular cartilage. Knee articular cartilage can be compared to the tread of an automobile tire, very durable but susceptible to wear over time. Osteoarthritis is the degenerative process, which results in the wearing out of this articular cartilage. As we age, the tread surface slowly erodes until the underlying bone is exposed. This exposed bone can be painful when the joint moves and bears weight.
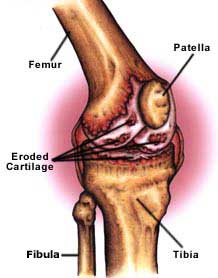
Osteoarthritis, or degenerative arthritis, is a wear and tear disease that affects knee articular joint cartilage. The cartilage is worn away, creating painful bone-on-bone contact. As osteoarthritis becomes more severe, the joint loses range of motion, becomes increasingly painful, and may stop responding to conservative non-surgical treatment. It is at this point that knee replacement surgery may become an option to restore joint movement and to reduce or eliminate pain.
The most common symptoms of osteoarthritis are:
Some of the most common treatments include pain medication, viscosupplementation injections, cortisone injections, physical therapy, shoe modifications, and bracing to help reduce joint pain and increase range of motion and assistive devices such as walkers, canes, or support braces. If a patient with osteoarthritis is overweight, weight-loss maybe recommended to reduce the amount of stress placed on the joints. When these treatments fail to alleviate the painful symptoms of osteoarthritis, joint replacement surgery maybe recommended.
No, there are several indications for total knee replacement including rheumatoid arthritis, arthritis resulting from previous injury to the bones in the joint, corrections of various bone deformities, or direct trauma to the joint.
Exercise is necessary for proper healing. Depending on your particular knee problem, physical therapy may begin between 24 and 48 hours after surgery. Formal physical therapy may begin in the hospital and continue as directed.
Diligent physical therapy, and a willingness to follow the post operative recommendations will promote a more complete recovery. Most patients should be able to walk unassisted and drive four to six weeks after surgery. After a thorough evaluation, activities such as golf, bicycling, and swimming may be resumed.
Dr. Delee will set a follow-up schedule for the first year after surgery to evaluate each patient's progress. Annual visits may be required thereafter. Complications can occur with knee implants, so followup examinations when you notice a change in symptoms can assist in evaluating any changes that may occur with your new joint.
There are risks assorted with total knee surgery, These vary based on your medical condition and will be discussed with you before surgery.
The purpose of a joint replacement is to help restore movement to a joint with reduced pain. Once a patient's pain is under control, he or she should be able to return to a more active lifestyle. Activities that could not be performed before surgery, such as climbing stairs, walking acceptable distances, or driving, may be resumed as directed after total joint replacement surgery. Our office has patients who would be willing to speak with you about their experiences before and after total joint replacement surgery.
The average age for joint replacement is 65-80 years; however, joint replacement is indicated at younger ages when other disease processes occur and over 80 years of age in a relatively healthy, and active patient.
Dr. Delee will set a follow-up schedule for the first year after surgery to evaluate your progress. You will be seen regularly thereafter.
Total knee replacement, also called total knee arthroplasty, uses metal alloy and polyethylene (plastic) components to resurface the bones in the joint. The implants are designed to re-create the shape of the bones in a healthy joint.
The end of the thighbone (femur) can be compared to a rocking chair. It has two distinct surfaces, or rockers, that contact the top of the shinbone (tiba). Each rocker is called a condyle, and there are two condyles at the end of the thighbone. The femoral component re-creates each rocker at the end of the thighbone. The top of the tibia is covered with a metal tray that is used to support a polyethylene plastic bearing. The polyethylene acts as the joint's cartilage, absorbing stress and providing smooth movement. The Patellar articular surface may or may not be replaced. If replaced the polyethylene on the back of the kneecap also provides smooth movement against the femoral component.
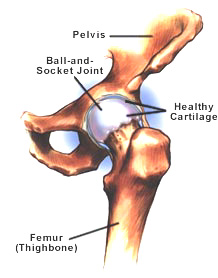
The healthy hip is a ball-and-socket joint. The ball is at the top of the thighbone (femur), and the socket (acetabulum) is in the hipbone (pelvis). This connection allows the leg to move in a wide variety of positions. The ball and socket are each covered with cartilage that lubricates and cushions the bones during movement. In the arthritic hip the articular cartilage is eroded, resulting in painful and limited motion, worsened by weight bering.
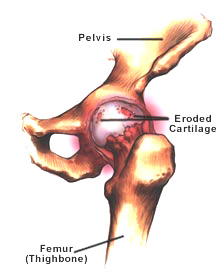
Osteoarthritis, or degenerative arthritis, is a wear and tear disease that affects joint articular cartilage. The articular cartilage is worn away, creating painful bone-on-bone contact. As osteoarthritis becomes more severe, the joint loses range of motion, becomes increasingly painful, and may stop responding to conservative non-surgical treatment. It is at this point that hip replacement surgery becomes an option for restoring motion to the affected joint.
The most common symptoms of osteoarthritis are:
Some of the most common treatments include assistive devices such as walkers or canes. If a patient with osteoarthritis is overweight, weight-loss may be recommended to reduce the amount of stress placed on the joints. Physical therapy may also be used to help reduce joint pain and increase range of motion. Pain medications and/or cortisone injections may also be used to reduce joint pain. When these treatments fail to alleviate the painful symptoms of osteoarthritis, joint replacement maybe recommend.
There are several indications for total hip replacement including rheumatoid arthritis, osteoarthritis, arthritis resulting from previous injury to the bones in the joint, various bone deformities, direct trauma to the joint (such as a fracture), and avascular necrosis (lack of blood supply that leads to bone death).
The average age for hip replacement is 65-80 years; however, hip replacement is indicated at younger ages when other disease processes occur and over 80 years of age in a relatively healthy, active patient.
Exercise is necessary for proper healing. Therapy is recommended to assist you with gentle leg movement, strengthening, and mobility exercises between 24 and 48 hours after surgery. Formal physical therapy may begin in the hospital and usually continues after discharge for approximately 6 weeks.
Patients with total hip replacement can typically participate in low-impact activities after surgery. Golf, walking, and swimming are a few examples of low-impact activities. Talk to Dr. DeLee before participating in any activity.
Yes.
Dr. Delee will set a follow-up schedule for the first year after surgery to evaluate your progress. You will be seen regularly thereafter. Complications can occur with implants, so when you notice a change in symptoms, call to be seen to assist in evaluating any changes that may occur with your new joint.
Yes, the risk of total hip replacement will very from patient to patient due to each patient's medical condition.
Diligent physical therapy, proper diet, and a willingness to follow all of the surgeon's recommendations will promote a more complete recovery after surgery. Most patients should be able to walk unassisted and drive from four to six weeks after surgery. However, each patient's recovery time may vary. After a thorough evaluation by the physician, activities such as golf, bicycling, and swimming may be resumed.
Most commonly, joint replacement recipients must avoid moving their hip greater than 90 degrees and sitting for long periods of time. It is also important to avoid crossing legs while sitting, standing, or lying down. Avoid sleeping on your side, bending at the waist, and pivoting or twisting your legs.
The bones in the hip are exposed by an incision approximately 6 to 8 inches long. The damaged sections of bone are removed to make room for the replacement components. The thighbone (femur) receives a metal alloy stem and ball and the pelvis receives a metal cup and liner. Traditionally, the metal cup is lined with polyethylene (plastic) to act as healthy cartilage. However, modern technology has allowed advancements in both metal and ceramic liners. These components now give the patient and surgeon additional options for hip replacement.
There are two types of cartilage in the knee. The first is fibrocartilage, which is seen in the meniscus. The second is the articular cartilage, which covers all bone surfaces in the knee joint. The function of articular cartilage is to provide a smooth, low-friction, weight-bearing surface that also acts to protect the underlying bone.
Articular cartilage is composed of very specialized cells called chondrocytes. Chondrocytes comprise less than 10% or articular cartilage dry weight. These cells reside in an extracellular matrix consisting of collagen, proteoglycan molecules, and water. There are many types of collagen, but the majority of collagen in articular cartilage is Type II. The proteoglycans are very large molecules that bind water. This accounts for the pressure, which makes cellular cartilage highly resistant to compressive loads. The chondrocytes provide the metabolic activity to maintain both the cartilage and the proteoglycans.
This complex structure of articular cartilage results in essentially no ability to repair itself. The poor healing response is due to a lack of blood supply in articular cartilage plus the inability of mature chondrocytes to migrate and reproduce into an area of damaged articular cartilage.
Articular cartilage damage can result from an acute injury or can be due to prolonged wear and tear. Acute injury usually results in lesions that are amenable to cartilage repair (or restoration). Routine wear and tear result in large areas of cartilage wear that are usually not amenable to articular cartilage restortation procedures.
An important part in the evaluation of patients with articular cartilage defects is determining which injuries are amenable to articular cartilage repair and which are not. Approximately 900,000 Americans suffer from articular cartilage injuries per year.
Many factors such as size of the injured area, patient's age, patient's level, and leg alignment, etc. are used to decide which procedure is utilized.
Dr. DeLee has experience in all types of cartilage restoration and provides state-of-the-art patient education, research, and surgical treatment.
Osteoarthritis, sometimes called degenerative arthritis or degenerative joint disease, is a condition that involves the breakdown of joint articular cartilage. Often the cause is unknown, but osteoarthritis may develop as a result of injury to the joint, excess body weight, or years of wear and tear on the joint articular cartilage. As joint cartilage wears away, the bone begins to make painful bone on bone contact. The early stages of osteoarthritis can be treated with a variety of conservative, non-surgical treatments. However, as the joint cartilage continues to wear away and the symptoms of osteoarthritis become more severe, surgery may be recommended to correct the damaged bone and cartilage.
Osteoarthritis develops slowly over several years. The symptoms of osteoarthritis are mainly pain, swelling, and stiffening of the knee. The pain of osteoarthritis is usually worse after activity. Early in the course of the disease, you may notice that your knee does fairly well while walking then after sitting for several minutes, the knee becomes stiff and painful. As the condition progresses, pain can interfere with even simple daily activities. In the late stages, the pain can be continuous and even affect sleep patterns.
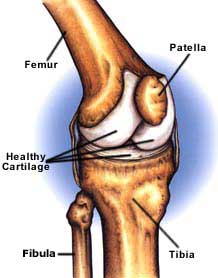
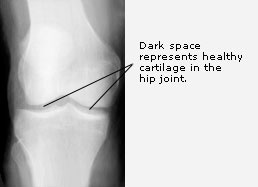
To diagnose osteoarthritis, a complete history and physical exam and a series of x-rays are taken. On an x-ray, a healthy knee joint has a space between the bones in the joint. Although you cannot see the cartilage on an x-ray, in the healthy knee, the cartilage is working to cushion and smooth the movement of the thighbone (femur) against the lower leg (tibia). On the x-ray of a knee with osteoarthritis, there is bone on bone contact because the articular cartilage between the femur and tibia has been worn away.

Unlike osteoarthritis, rheumatoid arthritis usually affects more than one joint at a time. The joints are affected by excess fluid and the synovial membranes, which are the linings of the joints. The normal function of the membranes is to produce synovial fluid, which lubricates and nourishes joint cartilage. With rheumatoid arthritis, the synovial tissue swells and leads to the destruction of bone and articular cartilage. The symptoms of rheumatoid arthritis vary, but many people experience painful joint swelling and progressively limited joint movement as the cartilage wears away.
Osteoarthritis is a condition, which progresses slowly over a period of many years. Osteoarthritis cannot be cured. Treatment is directed at decreasing the symptoms, and slowing the progress of the condition. There are a number of non-surgical treatments for osteoarthritis. Moderate doctor-prescribed exercise and physical therapy are excellent ways to keep your joints moving and to help relieve moderate joint pain. Joints that are not regularly exercised become tight and painful. Excess body weight places extreme amounts of pressure on the joints. If you are overweight, weight loss may be recommended to help relieve unwanted stress and pain on your joints.Assistive devices, such as a cane or a walker, can help reduce the pressure placed on joints and alleviate some pain. Resting after activity can also help control moderate joint pain. The treatment of osteoarthritis depends on how far advanced the condition is. In the early stages, treatment for osteoarthritis is usually directed at decreasing the inflammation in the joint. Anti-inflammatory medications, such as aspirin and ibuprofen, are useful in decreasing the pain and swelling from the inflammation. Sometimes a series of injections with a joint like fluid, a process called viscosupplementation will be beneficial. If the symptoms continue, a cortisone injection may be used to bring the inflammation under better control and ease your pain. Cortisone is a very powerful anti-inflammatory medication, but does have secondary effects that limit its usefulness in the treatment of osteoarthritis. The major drawback in the use of intra-articular injection of cortisone is the fact that it may actually speed the process of degeneration when used repeatedly. We use cortisone sparingly, and attempt to avoid multiple injections. There are also braces that can reduce the pressure on the side of the knee that is most involved. These braces have been designed mainly for the more common condition of early wear and tear in the medial compartment for the knee.
Arthroscopy may be useful in the treatment of osteoarthritis of the knee. Arthroscopy allows the surgeon to debride the knee joint. Debridement essentially consists of cleaning out the joint of all debris and loose fragments. During the debridement, any loose fragments of cartilage are removed, and the knee is washed with a saline solution. Debridement of the knee using the arthroscope can sometimes afford temporary relief of symptoms.
Osteoarthritis affects the inside half (medial compartment) of the knee more often than the outside (lateral compartment). This can lead to the lower extremity becoming slightly bow-legged, or in medical terms, a genu varum deformity. The result is that the weight bearing line of the lower extremity moves more medially (towards the medial compartment of the knee). (It's really all in the physics/biomechanics of the situation.) The end result is that there is more pressure on the medial joint surfaces, which leads to more pain and faster degeneration.
In some cases, re-aligning the angles in the lower extremity can result in shifting the weight-bearing line to the lateral compartment of the knee. This, presumably, places the majority of the weight-bearing force into the healthier compartment of the knee. The result is to reduce the pain and delay the progression of the degeneration of the medial compartment.
The procedure to realign the angles of the lower extremity is called a Proximal Tibial Osteotomy. In this procedure, a wedge of bone is removed from the lateral side of the upper tibia. This converts the extremity from being bow-legged to knock-kneed. This procedure is not always successful, and generally will reduce pain, but not eliminate it altogether. The advantage to this approach is that very active people still have their own knee joint, and once the bone heals there are no restrictions to activity level.
The Proximal Tibial Osteotomy in the best of circumstances is only a temporary solution. It is thought that this operation buys some time before ultimately needing to perform a total knee replacement. The operation usually lasts for 5-7 years if successful.
The ultimate solution for osteoarthritis of the knee is to replace the joint surfaces with an artificial knee joint. The decision to proceed with a total knee replacement is usually considered in people over the age of 60, (although younger patients sometimes require the surgery simply because no other acceptable solution is available to treat their condition). The main reason orthopaedic surgeons are reluctant to perform knee replacement on younger individuals, is that the younger the patient, the more likely the artificial joint will wear out. Replacing the knee the second and thrid time is much harder and much less likely to succeed.
Artificial knee joints last about 10 years in an elderly population. Younger patients are more active and place more stress on the artificial joint that can lead to loosening and failure earlier. Obviously, younger patients are also more likely to outlive their artificial joint, and will almost surely require a revision at some point down the road.
Total knee replacement, also called total knee arthroplasty, uses metal alloy and polyethylene (plastic) components to resurface the bones in the knee joint. The implants are designed to re-create the shape of the bones in a healthy joint.
The end of the thighbone (femur) can be compared to a rocking chair. It has two distinct surfaces, or rockers, that contact the top of the shinbone (tibia). Each rocker is called a condyle, and there are two condyles at the end of the thighbone. The femoral component re-creates each rocker at the end of the thighbone. The top of the tibia is covered with a metal tray that is used to support a polyethylene plastic bearing. The polyethylene acts as the joint's cartilage, absorbing stress and providing smooth movement. The Patellar articular surface may or may not be replaced. If replaced the polyethylene on the back of the kneecap also provides smooth movement against the femoral component.

